ACL: Reconstruction and Rehab
By Andrew Richardson
In this article I will be looking at the anatomy of the
knee, the ACL and its role, how does the ACL tear, the surgical procedure to
repair it. Then to finish the rehab protocol to get athletes back playing their
sport. I will be making reference to my day spent in SSC (Santry Sports Clinic)
in Dublin, where I learned a lot more about ACL’s and their own World Class
Return to Play Protocol.
Anatomy and Type of
Joint of the Knee
The knee joint joins the thigh with the leg and consists of two articulations: one between the femur and tibia, and one between the
femur and patella.[1] It is the largest
joint in the human body.[2]
The knee is a mobile trocho-ginglymus (a hinge joint), which permits flexion
and extension as well as slight internal and
external rotation. The knee joint is vulnerable to both acute injury and the
development of osteoarthritis.It is often grouped into tibiofemoral
and patellofemoral components.[3][4]
(The fibular collateral ligament is often
considered with tibiofemoral components.)[5]Below
are a few images of the knee from a range of angles (this will help understand the
terminology further on).
What is the ACL?
ACL stands for “Anterior Cruciate Ligament” and is one of
four ligaments that help to stabilise the knee joint through an array of
movements. A ligament is a very tough/strong band of tissue which its role (no
matter the location in the body) is to connect bones together at joint.
Ligaments are found at all joints. For the knee in this case it is the femur to
the tibia. The ACL is one of two ligaments that cross each other over deep
within the centre of the joint.
The front of the human body is known as the anterior and the
back is known as the posterior. The front ligament is called the ACL (Anterior
Cruciate Ligament) and at the back is the PCL (Posterior Cruciate Ligament).
The ACL is a very important structure as t helps with preventing the tibia (shin
bone) from sliding and rotating too much (prevents a large range of motion and
instability). It particular provides stability in twisting and turning actions.
The PCL prevents the tibia from moving backwards and is the less frequently
injured out of the two cruciate ligaments.
Then we have two ligaments at either side of the knee, they
are known as collateral ligaments. One is called the MCL (Medial Collateral
Ligament) as it’s on the inner side towards the body’s midline. The other is
called the LCL (Lateral Collateral Ligament) as it’s on the lateral side. These
ligaments provide the knee with stability during sideways motions.
How can the ACL tear?
The most common way the ACL can tear is through a
combination of sudden stopping motion on the leg while pivoting on the knee. In
70% of cases this happens during non-contact movement e.g. rapidly changing
direction, landing from a jump, an abrupt deceleration or twist. Particular
sports e.g. soccer, GAA, rugby and basketball commonly demand these activities
of the knee. Skiing is another common mechanism of cruciate injury and various
falling mechanisms have been described. A contact injury e.g. a rugby tackle or
road traffic accident is whereby the knee is forced excessively into a
stressful position by outside contact. An ACL tear can mean a range of things
as shown from the video https://www.youtube.com/watch?v=TSMA5EQZuTk
Here is an example of an ACL tear;
What other Knee
structures can be injured when the ACL tears?
Approximately half of all ACL injuries will be isolated.
This means many patients injure another knee structure at the same time. These
include the meniscal cartilage, the articular cartilage surface and other
ligaments around the knee. Any additional damage will be identified on MRI and
confirmed during surgery. Some of these cartilage tears can be left alone but
some require treatment with either partial removal or repair. Some injuries
require time to heal pre surgery, whereas other such injuries are addressed
during surgery.
How will my Knee
function if the ACL is torn?
It is possible to function without your ACL. If you have
appropriate lower limb strength and control then low level activities are
possible. Young athletes and athletes looking to return to sports involving
twisting, turning and landing will most likely require reconstruction. Return
to these higher level sporting activities is the principle indication for ACL
reconstruction.
Repeated unstable episodes are to be avoided as it increases
the likelihood for cartilage damage in the knee and increases wear and tear in
the longer term. ACL reconstruction offers excellent stability and outcomes on
return to sport for athletes who are motivated and compliant with the
rehabilitation programme.
ACL surgery
An individual embarking on ACL reconstruction should have an
understanding of the procedure and fully commit to the rehabilitation process.
The operation involves replacing the torn ACL with a graft taken from another
part of the knee. The aim is to positon this graft within the knee to take the
place of the torn ACL and mimic its stabilising function. The two most commonly
used grafts are constructed from either the patellar tendon or the hamstring
tendons. The graft chosen will vary according to the patient and depends on
other injuries, sports occupation and individual anatomical variations. The
majority of the operation is performed arthroscopically (key hole surgery).
Remember surgery is not the only option for a torn ACL: https://www.youtube.com/watch?v=6zN-C-4nayw
However an incision is required to harvest the graft over
the front of the knee. During surgery any other structures damaged during the
injury will also be repaired. While viewing the inside of the joint through
arthroscope, guides are used to drill bony tunnels to allow placement of the
graft. The graft is then pulled into these bone tunnels and spans the knee
joint. Screws are placed to wedge the graft against the wall of the tunnels to
give immediate stability and allow healing of the new graft. This early bonding
of the graft takes approximately 6 weeks for patellar tendon grafts and 10
weeks for hamstring tendons. The graft is strong enough at 6 months post-surgery
to withstand load associated with sporting movement but continues to mature
over the course of the following 6-12 months.
You’re Role in
Rehabilitation
It is important to follow the RICE regime following your
injury (Rest, Ice, Compression and Elevation)
-
Rest: Reduce your activity levels for the next
2-5 days depending on the level of your injury. This minimises the chance of
further tissue damage facilitates healing of the injury.
-
Compression: Your knee may be supported by a
dressing during the day, which should be taken off when exercising and at night
time.
-
Ice: Ice is an effective means of decreasing
swelling and pain and can be used as long as you have swelling. Use a cold gel
pack or ice cubes in a bag. Apply the ice to the affected joint, with the leg
elevated. Apply the ice for 20-30 min max, then reapply every 2 hours.
-
Elevation: Lying down, elevate the joint above
the level of the heart as much as possible in the initial 72 hours of injury.
Restoring your ROM
Restoration of full knee extension and as much flexion as
possible is important as this facilities normal gait and movement. This can be
achieved by working on the appropriate exercises as tolerated.
Gait
Due to pain, reduced proprioception ROM, muscular strength
and control, we can have altered or compensatory movement. While it important
to RICE the knee you are encouraged to walk with a normal gait pattern as early
as possible (crutches may be necessary initially) starting with short distances
and progressing as tolerated. Gait refers to walking pattern
Normal Gait
Improving Neuromuscular
Control and Strength
As with any knee injury, pain and swelling in the knee are
associated with muscle inhibition (reduced muscle function) and loss of
proprioception/control. Sufficient strength and control around the hip and knee
are vital to support the knee and thus avoid excessive load through the joint. Appropriate
strength (based on symmetry and body weight) in the quadriceps/hamstrings and
optimal single leg control are an important component of a pain free return to
performance. Therefore any improvements that will improve strength and control
pre surgery, will facilitate faster recovery times following surgery.
Video on neuromuscular training for ACL rehab: https://www.youtube.com/watch?v=V7alxsuQxIE
Mental Preparation
Mental preparation prior to surgery plays an important role
in your rehab. It is based on your education and knowledge of both the surgery
and the rehabilitation process and what a fully rehabilitated athlete returning
to sport looks like. A good understanding will enable you to set realistic
goals with your physiotherapist both pre-operatively and postoperatively.
Focusing on short term goals on what you can achieve between diagnoses and
having surgery will be very beneficial. Positive self-talk regarding the successful
outcome and return to sport as well as imagery of returning to play can assist
during this period as well.
Individuals will have a different response to surgery post
operation so psychological support needs to be provided and individualised to each
person: https://www.youtube.com/watch?v=scgoZ9l7VMY
Exercise Programme
These exercises are to be done prior to your surgery (all
done with light weights and or no weights)
-
Knee Extension
-
Knee Flexion
-
Straight Leg Raise
-
Single leg Chair Squat
-
Leg Press
-
Hamstring Curl
-
High Knee Walking
-
Single Leg Balance
Exercises shown below
As a coach the athlete/client puts their trust in you. They
are paying for a service to get them back playing to the same level as before in
a quick time period. Trust is key between you and the athlete: https://www.youtube.com/watch?v=aoKwQH04KXk
MRI and ACL
Here is a good short video on how to read an MRI and to see
if you have torn an ACL
SSC ACL
Rehabilitation Pathway
In my professional opinion after spending a day at SSC I can
honestly say this is the best protocol for a successful ACL
reconstruction/rehabilitation programme out there (that I have seen). It
combines the fields of Strength and Conditioning, Physio, Biomechanics and
Surgery all under one roof for each individual patient.
I saw an integration of the above fields all corresponding
with each other which is fantastic for the athlete but also accelerates
research and CPD for all the fields in the facility.
Components of a
Successful ACL Rehabilitation Programme at SSC
Single
Leg Neuromuscular Control + Full ROM (Range of Motion) + Strength/Power
Running + Turning +
Training = Graduated Return to Performance
ACL Rehabilitation
Pathway
Stage 1: Rehabilitation
What’s involved?
-
Education on the rehab process
-
Assessment of your gait
-
Assessment of knee joint ROM and strength
-
Assessment of single leg control
-
Provision of prehabilitation exercises and
pre-operative advice
-
Outline of what to expect during your in-patient
stay and during the early stages of rehab
Stage 2: Post-Operative Inpatient Rehabilitation
What’s involved?
-
Assessment of the knee
-
Completion of post-operative rehabilitation
exercises
-
Gait practice with crutches
-
Completion of stairs assessment
-
Discharge paperwork for your physiotherapist who
you will see within 7-10 days of discharge
-
Review the ACL Rehabilitation pathway and outline early rehabilitation phase
-
Answer any questions you may have about the
surgery, rehabilitation and biomechanical reviews.
Stage 3: Initial 2Dimensional (2D) ACL Review
What’s involved?
-
Feedback on your rehabilitation to date
-
Assessment of knee joint range of motion
-
2D motion analysis of Single leg Control
-
Isokinetic Strength testing of the quadriceps and
hamstring muscle
-
Mid-Thigh pull to assess strength through the kinetic
chain
-
Single leg vertical jump height
-
Progress report for you, your consultant and physiotherapist
-
Overview of 6 Month 3D testing protocol
Stage 4: 3 Dimensional (3D) Biomechanical ACL Review
What’s involved?
-
Review of your rehabilitation progress to date
-
Assessment of knee joint range of motion
-
3D motion analysis of single leg control and
sports specific movement including indecision testing using Smartspeed gate
system
-
Isokinetic and mid-thigh pull strength testing
-
Single leg vertical and horizontal jump
profiling
-
Progress report for you, your consultant and physiotherapist
Stage 5: Final 3D Biomechanical Review
What’s involved?
-
This testing process will mirror that of the 6
month protocol ideally placing you in the best position for a successful return
to your chosen sport and completion of the rehabilitation process. You will be advised
on how to resolve any remaining deficits and maintain healthy and high
performing knees.
ACL
Research
Some of my favourite ACL related journals;
-
Torg, J. S., Conrad, W., &
Kalen, V. (1976). Clinical I diagnosis of anterior cruciate ligament
instability in the athlete. The American journal of sports medicine, 4(2),
84-93.
-
Shelbourne, K. D., & Nitz, P.
(1990). Accelerated rehabilitation after anterior cruciate ligament
reconstruction. The American journal of sports medicine, 18(3),
292-299.
-
Hewett, T. E., Myer, G. D., Ford,
K. R., Heidt, R. S., Colosimo, A. J., McLean, S. G., ... & Succop, P.
(2005). Biomechanical measures of neuromuscular control and valgus loading of
the knee predict anterior cruciate ligament injury risk in female athletes a
prospective study. The American journal of sports medicine, 33(4),
492-501.
ACL’s and
Powerlifting
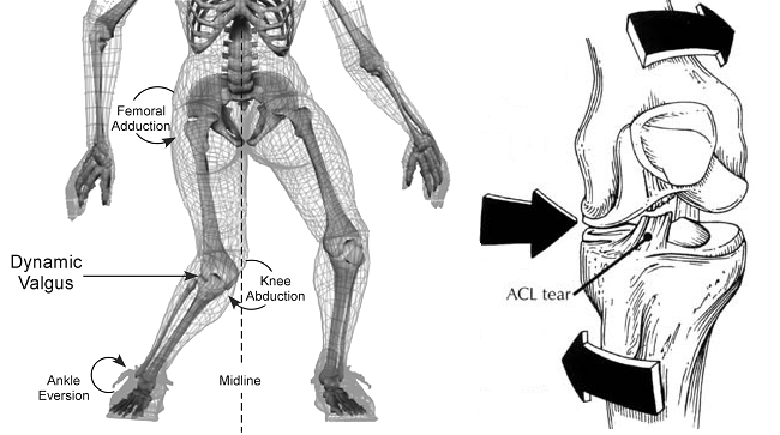
Now to apply this to Powerlifiting. The only exercise which
poses the greatest risk of an ACL tear is during the squat through a knee
valgus collapse.
Now during an ACL rehab all clients are made to do squats as
part of their rehab protocol which is good. All of them keep a neutral foot
positon for quad activation and to help speed up recovery. Looking at
powerlifters and weightlifters a lot external rotate their feet so it activates
the hamstrings more/glutes more. This is fine for the sport but for rehab
purposes it should be gradually phased in.
For rugby/sprinting/soccer etc no external rotation just
neutral foot position then work to isolate the glutes and hamstrings on their
own. Over time once (7 months plus) introduce a slight external rotation to strengthen
that plane of motion.
Work on building up the knee valgus and all quadriceps muscles.
This takes priority. Use close stance box squats at start then build this up
through increasing weight and increasing the ROM of the squat.
Concluding
Thoughts
So you now know about the Knee anatomy, ACL, ACL tear, rehab
process, SSC in Dublin and ACL research.
I hope this helps everyone in their rehab
Regards
Andrew
References
2.
Jump up ^ Kulowski,
Jacob (July 1932). "Flexion
contracture of the knee". The Journal of Bone & Joint Surgery 14
(3): 618–63. Republished as: Kulowski, J (2007). "Flexion
contracture of the knee: The mechanics of the muscular contracture and the
turnbuckle cast method of treatment; with a review of fifty-five cases.
1932". Clinical orthopaedics and related research 464: 4–10. doi:10.1097/BLO.0b013e31815760ca
(inactive 2015-05-08). PMID 17975372.
6.
Santry Sports Clinic: ACL Rehabilitation Pathway
7.
Santry Sports Clinic: ACL Rehabilitation
Programme
AAndrew Richardson, Founder of Strength is Never a Weakness Blog
I have a BSc (Hons) in Applied Sport Science and a Merit in my MSc in Sport and Exercise Science and I passed my PGCE at Teesside University.
Now I will be commencing my PhD into "Investigating Sedentary Lifestyles of the Tees Valley" this October 2019.
I am employed by Teesside University Sport and WellBeing Department as a PT/Fitness Instructor.
My long term goal is to become a Sport Science and/or Sport and Exercise Lecturer. I am also keen to contribute to academia via continued research in a quest for new knowledge.
My most recent publications:
My passion is for Sport Science which has led to additional interests incorporating Sports Psychology, Body Dysmorphia, AAS, Doping and Strength and Conditioning.
Within these respective fields, I have a passion for Strength Training, Fitness Testing, Periodisation and Tapering.
I write for numerous websites across the UK and Ireland including my own blog Strength is Never a Weakness.
I had my own business for providing training plans for teams and athletes.
I was one of the Irish National Coaches for Powerlifting, and have attained two 3rd places at the first World University Championships,
in Belarus in July 2016.Feel free to email me or call me as I am always looking for the next challenge.
Facebook: Andrew Richardson (search for)
Facebook Page: @StrengthisNeveraWeakness
Instagram: @arichiepowerlifting
Snapchat: @andypowerlifter
Email: a.s.richardson@tees.ac.uk
Linkedin: https://www.linkedin.com/in/andrew-richardson-b0039278